Dr. Rice has joined Beacon Orthopedics and Sports Medicine
Congratulations Dr. Rice: 2025 Cincinnati Magazine Top Doctor



Acetabuloplasty (a.k.a. "Pincer takedown")
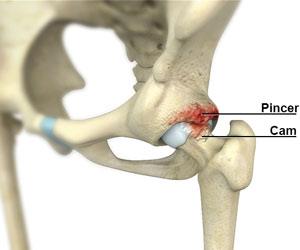
The hip joint is a ball and socket joint, formed by the upper rounded end (head) of the femur (thigh bone) that articulates with the cavity of the acetabulum in the pelvic bone. The smooth surfaces of the femoral head and acetabulum allow smooth movement of the hip joint. Occasionally, the acetabulum and/or the femoral head may have bony irregularities due to disease, overuse or growth abnormalities, and is called femoroacetabular impingement (FAI). This can cause damage to the cartilage and tissues that border the articulating surfaces, resulting in pain and limitation of movement. FAI associated with the acetabulum is called Pincer impingement. An acetabuloplasty is a surgical procedure that corrects Pincer impingement and is indicated when conservative treatments fail to relieve pain.
Acetabuloplasty is usually performed by arthroscopy, a minimally invasive technique in which a camera and miniature instruments are inserted through small incisions over the hip to reach and correct abnormalities in the acetabulum. The over-coverage, or pincer lesion, is trimmed with a burr and the acetabulum reshaped to facilitate normal hip movement. The re-sculpting is often subtle, typically requiring only a few millimeters of resection. Any labral damage is also repaired. The incisions are then sutured.
Following the surgery, patients return home the same day. Crutches are typically needed for 4 weeks after surgery. Physical therapy is usually recommended immediately following surgery to improve movement and strength.
Complications with acetabuloplasty are rare, and may include nerve damage, bleeding, over- or under-resection of the abnormalities. Over-resection is among the most dreaded complication, as it can lead to iatrogenic instability and is not easily corrected.
Frequently Asked Questions
- How do I decide if I need acetabuloplasty surgery?
- The need for acetabuloplasty is often an individualized decision based on complex imaging data from plain x-rays and often MRI and/or CT images. In Dr. Rice’s practice, the most common pincer lesion warranting acetabuloplasty is focal, in the anterior-superior quadrant, and creates a “crossover sign” on xray, but may be more challenging to appreciate on MRI studies, where focal pincer lesions are often missed.
- How does a preoperative CT scan help with acetabuloplasty surgery?
- Preoperative CT scans are routine for Dr. Rice’s patients undergoing hip arthroscopy, as the 3D reconstructed images reveal tremendous detail and help define the exact borders of the pincer lesion, as well as depth.
- If I am undergoing hip labral repair surgery, does acetabuloplasty change my recovery?
- In Dr. Rice’s practice, the addition of acetabuloplasty to hip labral repair surgery does not significantly change the amount of time on crutches or the overall recovery timeline and return to sport. Regardless, crutches are used 4 weeks with 50% weight-bearing. By debriding the bone to a healthy bleeding surface, the acetabular rim after acetabuloplasty is thought to provide the optimal healing environment for the repaired labrum. In this sense, acetabuloplasty has a beneficial and synergistic effect when combined with labral repair.
For more FAQs, see cincysportssurgeon.com/fai-faq-sports-medicine-orthopedic-surgeon.html
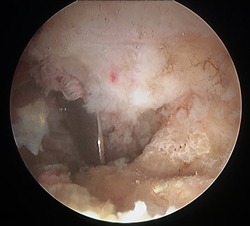
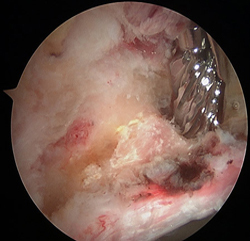
Pincer lesion untreated
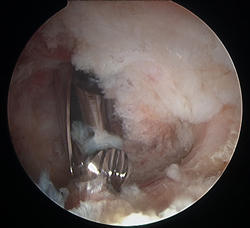
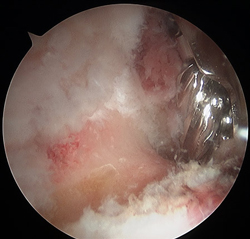
Acetabuloplasty to resect pincer lesion
Pincer lesion in young active individual with pain during yoga and pilates activity, failed nonsurgical treatment
Acetabuloplasty completed to correct pincer lesion. Patient successfully returned to yoga and pilates with no pain or dysfunction
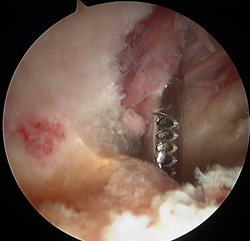
Hip Scope Labral Repair
nodisplay
nodisplay
Hip Procedures
- Hip Arthroscopy
- Labral Repair
- Acetabuloplasty (a.k.a. "Pincer takedown")
- Microfracture
- Femoroplasty (a.k.a. "CAM takedown")
- Synovectomy
- Ligamentum Teres Tear Debridement
- Iliopsoas Recession
- Subspine Impingement Decompression
- Endoscopic Abductor Tendon Repair
- Endoscopic ITB Release
- Endoscopic Bursectomy
- Proximal Hamstring Repair
- FAI FAQs
- Ischiofemoral Endoscopic Decompression